
Prof. Jennifer Morton, Cancer Research UK Scotland Institute
In our previous article, we introduced the origins of the KPC cell line, developed by Professor Jennifer Morton at Cancer Research UK’s Scotland Institute. Here we focus on what matters most: how the KPC line is being used to answer some of the toughest questions in pancreatic cancer. From modelling metastasis and tumour-immune interactions to testing therapeutic strategies in immunocompetent systems, the KPC cell line offers a transplantable, genetically defined model that combines biological relevance with experimental flexibility. The studies highlighted below show why KPC has become a preferred platform for researchers who need to move efficiently between in vitro perturbations and immunocompetent in vivo validation.
From foundational models to practical experimental tools
The original KPC genetically engineered mouse model transformed pancreatic cancer research by revealing key drivers of tumour progression, stromal remodelling, and immune suppression. Today, scientists across the world are building on these foundational insights through the transplantable KPC-derived cell line established by Prof. Jennifer Morton at the Cancer Research UK Scotland Institute, which allows these key biological questions to be explored with greater experimental flexibility.

The KPC model enables defined genetic perturbation and functional analysis; here, PTEN loss increases macropinocytic uptake of fluorescent dextran (red) (adapted from Michalopoulou et al.).
By separating tumour genetics from tumour initiation, a key limitation of spontaneous models, the KPC cell line allows researchers to control timing, introduce defined perturbations, and apply treatments reproducibly, while still working in immunocompetent hosts. Compared with spontaneous models, they enable tumour genetics, timing, and treatment to be manipulated independently, supporting experiments that would otherwise require lengthy breeding strategies.
What began as a tool to study tumour biology in a more controlled way has since evolved into a platform for tackling increasingly complex questions, from adaptive resistance to treatment delivery and tumour–immune dynamics. Here is why researchers are extending the original vision of the model in practice.
Using the KPC line to study tumour adaptation
Tumour adaptation is a core reason why many targeted therapies fail; understanding it can guide more effective combinations.
A central challenge in pancreatic cancer research is understanding how tumour cells adapt when key signalling or metabolic pathways are disrupted, particularly as such adaptation often underlies therapeutic resistance. In spontaneous models, introducing additional genetic changes or systematically testing resistance mechanisms often requires long timelines. Several groups have therefore chosen the KPC cell line as a genetically defined but tractable baseline for studying tumour adaptation under selective pressure, such as pathway inhibition and nutrient stress.
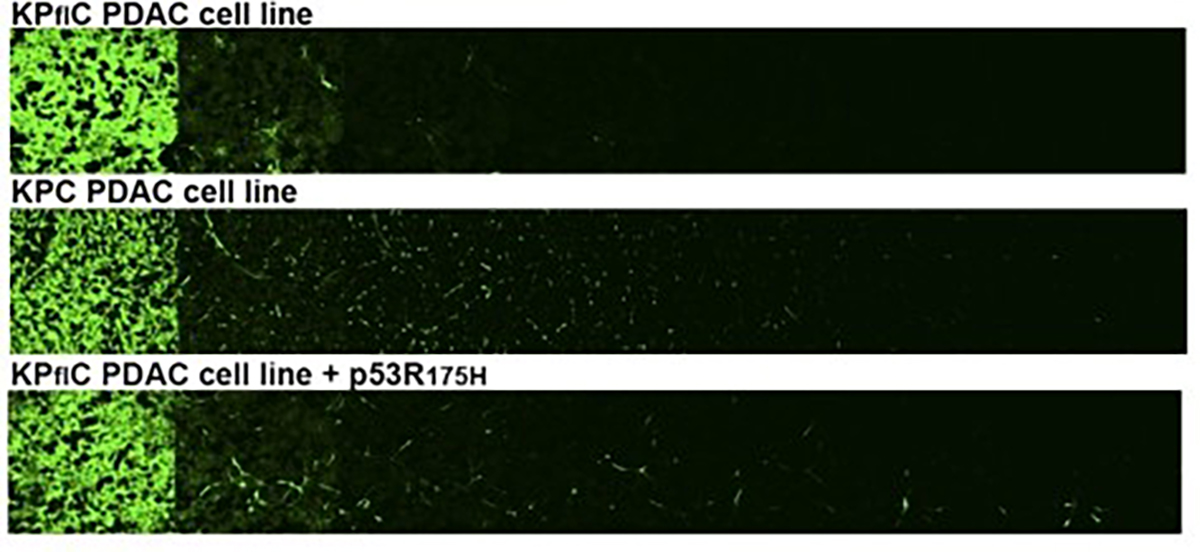
At the Cancer Research UK Scotland Institute (formerly the Beatson Institute), Michalopoulou and colleagues compared KPC and KCPTEN pancreatic cancer cell lines derived from genetically engineered mouse models to examine how PTEN loss reshapes nutrient uptake and influences response to mTOR inhibition. By combining in vitro metabolic and uptake assays with mechanistic perturbations, the team showed that PTEN loss enhances macropinocytosis, a process by which cells engulf extracellular material, allowing tumour cells to scavenge extracellular protein and sustain growth despite mTOR inhibition. This mechanism could be pharmacologically targeted by inhibiting lysosomal degradation, revealing a therapeutic vulnerability.
Related studies from multiple universities have used KPC-based perturbation models to examine tumour adaptation under defined genetic or treatment pressure, including circadian clock disruption shaping tumour growth in vivo and chemotherapy response (Schwartz et al.). Orthotopic KRAS-driven syngeneic models, in which tumour cells are implanted into the pancreas of immunocompetent genetically matched mice, have likewise been used to interrogate tumour–stroma signalling under defined perturbation. For example, genetic and pharmacological targeting of the ACSL3–PAI-1 axis reshaped fibrosis and altered immune cell infiltration in vivo (Sebastiano et al.). Disrupting mechanosensing pathways has shown how the physical properties of the tumour environment can influence fibroblast behaviour and tumour growth in vivo (Romac et al.).
Taken together, these studies show how the KPC cell line provides a controlled starting point for layering defined genetic or pharmacological perturbations and tracking tumour behaviour over time in vivo. By enabling rapid genetic engineering, quantitative metabolic and uptake assays in vitro, and validation in vivo, including syngeneic contexts, this approach allows researchers to interrogate how pancreatic cancer cells adapt under selective pressure without the constraints of spontaneous tumour development.
While the work above focuses on tumour-intrinsic mechanisms of adaptation, the same experimental flexibility can allow you to ask how treatment context itself—such as timing, delivery, or local intervention—shapes tumour response, helping you design experiments with improved translational impact.
Using KPC to test therapies in realistic in vivo contexts
How and when you deliver a therapy can be as important as the therapy itself, and transplant models let you study that explicitly.
Many clinically relevant questions in pancreatic cancer depend not only on which therapy is used, but also on when, where, and how it is delivered – factors that can substantially influence treatment outcome. Spontaneous tumour models can make such questions difficult to address, as tumour onset and progression are less predictable. By contrast, the KPC cell line allows tumours to be generated with defined timing and location, enabling researchers to align tumour growth more directly with treatment delivery and experimental intervention.
At the University of Glasgow, Falcone and colleagues used the KPC line to generate subcutaneous tumours in immunocompetent mice and examined how dietary serine and glycine availability influences radiotherapy response. By controlling both diet and radiation exposure, the group showed that amino-acid restriction increased response to radiotherapy. Rather than focusing on immune mechanisms directly, the study highlighted how systemic context, such as diet, can shape tumour response in ways not captured by standard in vitro assays.
Additional studies have applied orthotopic KPC tumour models to reconstruct clinically relevant intervention scenarios under controlled conditions, including local ablative therapy using irreversible electroporation (Woeste et al.).

The orthotopic KPC model enables testing of combination therapies in immunocompetent mice; here, β-glucan combined with irreversible electroporation reduces tumour burden (Woeste et al.).
In these settings, researchers use KPC-based transplantation models not to discover new driver mutations, but to model treatment delivery and response under controlled conditions. By combining syngeneic or orthotopic tumour implantation with defined local or systemic interventions and longitudinal assessment, KPC models allow researchers to examine how treatment design, local control, and host context influence tumour progression in immunocompetent hosts. This level of experimental control enables interrogation of tumour behaviours, such as host immune responses and tumour microenvironment dynamics, that depend on interactions with an intact host environment and are not readily captured in vitro.
If your work involves testing treatment timing, delivery, or combination strategies in vivo, the KPC cell line provides a way to do so within a defined genetic background and immune-competent setting, without the variability and timelines associated with spontaneous models.
Using KPC to model immune-dependent tumour behaviour in vivo
Interactions between tumour cells and the immune system are fundamentally different in vivo than in vitro, and models that capture this are essential for immunotherapy research.
Some tumour behaviours in pancreatic cancer are fully revealed when tumour cells interact with an intact immune system in vivo. To address biological questions that cannot be resolved in vitro, several groups have applied the KPC cell line as syngeneic allografts in immunocompetent hosts.
At the University of Glasgow, Newman and colleagues used parental and IDO1-engineered KPC cell lines to examine how immune-derived interferon-γ influences tumour metabolism in vivo. By implanting these lines into immunocompetent mice, the team showed that interferon-γ induces high IDO1 expression, activating the kynurenine pathway and enabling tumour cells to channel tryptophan metabolism into nucleotide biosynthesis. This immune-conditioned metabolic dependency was not apparent under standard culture conditions and emerged in the presence of host-derived signals.
Beyond tumour-intrinsic metabolic adaptation, KPC-derived tumours have also been used to interrogate immune behaviour that emerges only in immunocompetent hosts. Orthotopic KPC models have been used to demonstrate trained innate immunity within the pancreatic tumour microenvironment (Geller et al.), to show that local ablative therapy can further remodel myeloid activation states in vivo (Woeste et al.), and to reveal that microbiota-derived metabolites can influence chemotherapy response via neutrophil-derived myeloperoxidase (Tintelnot et al.). Together, these studies illustrate how host context and treatment exposure reshape tumour–immune interactions in ways not apparent under standard culture conditions and that depend on intact immune competence.

Orthotopic KPC-derived tumours in immunocompetent C57BL/6 mice, illustrating in vivo treatment-associated changes assessed by histology (Tintelnot et al.).
In these examples, the KPC cell line bridges reductionist systems and physiological complexity, allowing you to examine tumour-intrinsic processes within an immune-competent environment, while maintaining precise control over tumour genetics and timing.
Interpreting results and experimental caveats – why careful model interpretation matters!
As with any transplantable system, careful interpretation of data generated using the KPC cell line is essential. Studies have shown that additional genetic modifications, such as reporter gene expression, can alter tumour–immune interactions in immunocompetent hosts. For example, luciferase-expressing KPC tumours, in which a foreign reporter protein is introduced, have been shown to provoke immune responses that influence tumour growth dynamics in immunocompetent hosts (Ferrari et al.).
More broadly, the KPC cell line is most powerful when used alongside complementary models: it offers speed, experimental control, and accessibility that are difficult to achieve with spontaneous tumours, while necessarily sacrificing aspects of tumour initiation and long-term evolution. For researchers, this translates into faster hypothesis testing and greater experimental precision, with the option to validate findings in more complex models when needed.
Looking ahead
Across these examples, a clear pattern emerges: researchers are applying the KPC cell line not as simplified stand-ins, but as enabling platforms for asking nuanced experimental questions.
As research priorities increasingly focus on combination therapies, adaptive resistance, and tumour–microenvironment interactions, the KPC cell line provides a practical and experimentally accessible system for interrogating these challenges under controlled conditions. Its ability to bridge defined in vitro perturbations with immunocompetent in vivo validation positions it as a foremost platform for shaping preclinical pancreatic cancer research.
Explore the KPC cell line and see how this model can accelerate your next pancreatic cancer study
References
Falcone M et al. 2022. British Journal of Cancer. 127:1773–1786. PMID: 36115879.
Ferrari DP et al. 2024. Sci Rep. 14(1):13602. PMID: 38866899.
Geller A et al. 2022. Nature Communications. 13(1):759. PMID: 35140221.
Michalopoulou E et al. 2020. Cell Reports. 30(8):2729–2742.e4. PMID: 32101748.
Newman AC et al. 2021. Mol Cell. 81(11):2290–2302.e7. PMID: 33831358.
Romac JMJ et al. 2025. JCI Insight. 10(23):e196280. PMID: 41100488.
Schwartz PB et al. 2023. PLoS Genet 19(6): e1010770. PMID: 37262074.
Sebastiano MR et al. 2020. Sci. Adv. 6(44):eabb9200. PMID: 33127675.
Tintelnot J et al. 2023. Nature. 615(7950):168-174. PMID: 36813961
Woeste MR et al. 2023. J Immunother Cancer. 11(4):e006221. PMID: 37072351.