Case study on research by Elliott et al. 2026 iScience DOI: 10.1016/j.isci.2026.115839
Twenty years without progress
Few cancers have proven as resistant to therapeutic progress as glioblastoma (GBM). Despite two decades of intensive molecular characterisation – bulk transcriptomic subtyping, single-cell atlases, spatial mapping of tumour ecosystems, clinical outcomes have barely shifted since temozolomide became standard of care in 2005. The gap between molecular insight and treatment benefit is the central frustration of the field, and it reflects GBM’s defining feature: a tumour that looks different not only from patient to patient, but from cell to cell within the same mass, and that can shift its identity again under the pressure of treatment.
That heterogeneity is also why so many drug discovery efforts stall before they reach the clinic. A compound that performs well against one well-behaved cell line in a 2D dish often fails to generalise once it meets the diversity of a real tumour. Many commonly used GBM models represent only a narrow slice of the disease or diverge from patient tumours over time. And many models do not retain the glioblastoma stem cell (GSC) populations thought to underlie resistance and relapse. Even where stem-like features are retained, experimental formats can limit scale and consistency. The result is a disconnect between what is measured in screening and what happens in the clinic.
A different starting point

We spoke to Neil Carragher from the University of Edinburgh about his latest study in iScience, a phenotypic drug discovery screen on patient-derived glioblastoma stem cell models. He explained that teams using standard older models of GBM might be failing to identify biologically relevant targets:
“They will most likely uncover drugs and targets effective against highly proliferating cells that have adapted to high serum-containing in vitro conditions that poorly represent patient disease. It is likely that such drug-target mechanisms will not be as potent against heterogeneous GBM stem cell populations, which contribute to drug resistance and relapse.”
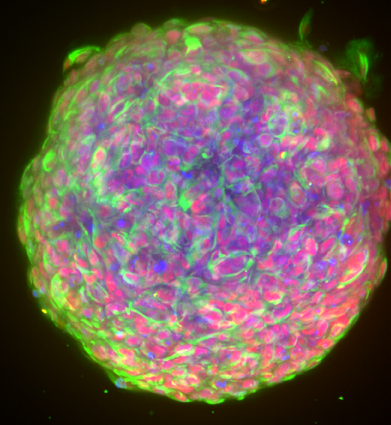
In their study, Neil and his team directly address the heterogeneity issue at the heart of GBM by building their screening campaign around six patient-derived GSC lines from the Glioma Cellular Genetics Resource (GCGR), a biobank of well-characterised, patient-derived GSC lines maintained under serum-free conditions on laminin. As the cells were cultured in this way, the lines preserved their stem-like properties and grow adherently, making them compatible with high-throughput formats. The models selected in this study covered the three major transcriptomic subtypes of GBM: classical, mesenchymal and proneural.
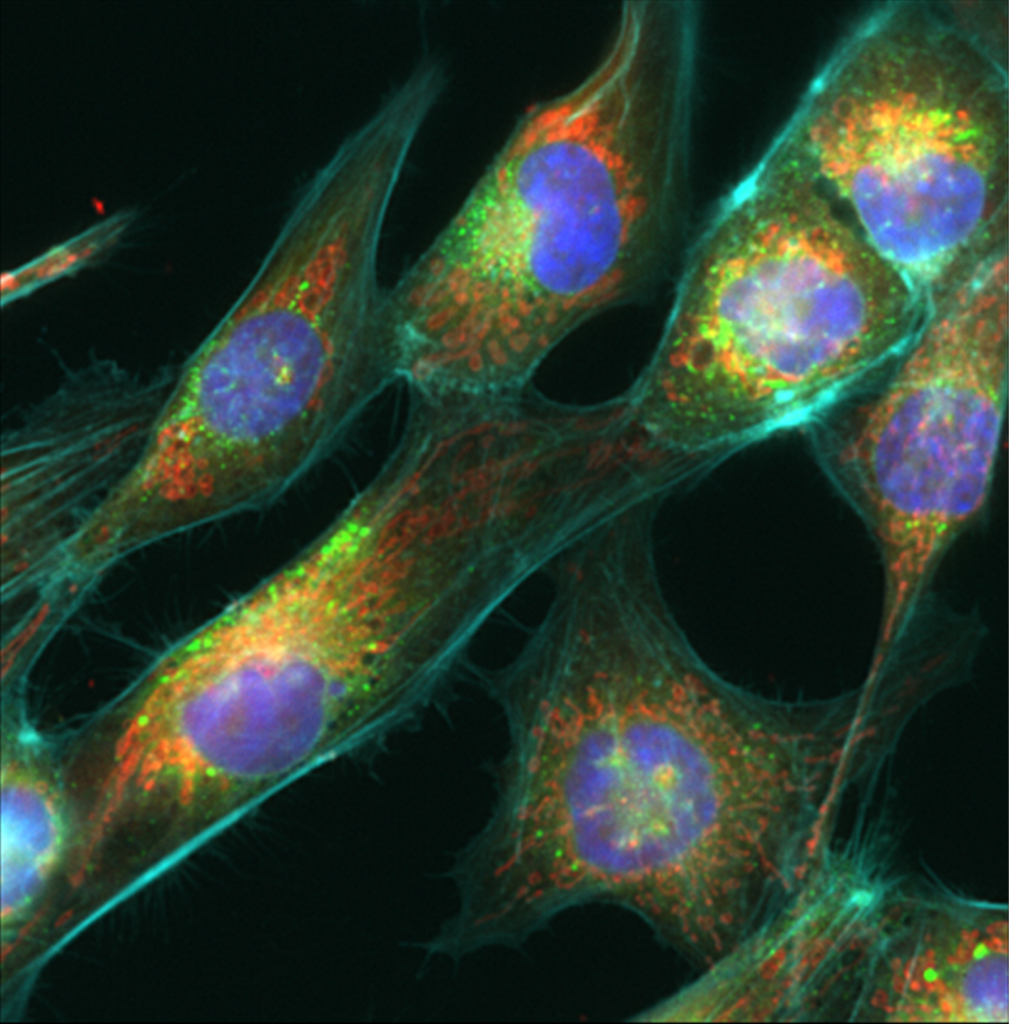
In this phenotypic screen, compounds were assessed using a Cell Painting assay, which is a multiplexed imaging approach that captures the morphological changes across nuclei, mitochondria, the endoplasmic reticulum, the cytoskeleton and the cell membrane simultaneously. This results in a richer readout than just cell viability, allowing identification of mechanistically distinct compounds.
The screening set in this study encompassed 3,866 compounds including FDA approved drugs, Phase I clinical candidates, selective chemical probes and the Kinase Chemogenomic Set (KCGS) – a curated collection of highly selective kinase inhibitors. Screening across all six GCGR cell lines in parallel meant that selectivity and breadth of activity could be assessed from the outset of the study, as opposed to a factor to follow-up with downstream.
According to Neil, screening across a heterogenous panel reveals much more than can modelled with a single cell line. On using a screen Neil said:
“This allows us to identify drug mechanisms-of-action which overcome the remarkable heterogeneity observed between GBM stem cells – that will hopefully identify treatments that will benefit a wider population of GBM patients. We can also correlate phenotypic response with genetic and proteomic data available on each cell line to identify predictive biomarkers of response to guide future personalised medicine strategies”.
What the screen found
From 3,866 compounds screened, 211 primary hits were identified and 164 confirmed in seven-point dose–response validation. The validated set spans a wide range of target classes: cell adhesion kinases (FAK, SRC), transcriptional regulators (HDAC, CDK9, BRD), MAPK pathway components (MEK1/2, PAK4/6), DNA damage and repair (PARP, TOPO), metabolism (FASN, NAMPT) and protein homeostasis (HSP90, VCP/p97).
Two target classes were characterised in depth. HDAC inhibitors showed consistent low-nanomolar activity across all six GSC lines; fimepinostat, a dual HDAC/PI3K inhibitor currently in phase II trials for paediatric brain tumours – was the most potent compound identified, with IC₅₀ values below 20 nM across the full panel. CDK9 inhibitors showed even more rapid effects: selective agents NVP-2 and AZD4573 produced broad suppression of cell cycle, DNA damage response, PI3K-AKT and MAPK signalling within 24 hours, alongside rapid induction of apoptosis that was independent of CDK1/2 inhibition.
One of the more clinically significant observations concerns MEK inhibitors. Several compounds showed strong activity in half of the GSC lines tested, but this pattern did not correlate with BRAF or NF1 mutation status – the biomarkers currently used to stratify patients for MEK inhibitor trials. This raises the possibility that existing trial designs may be failing to capture the full spectrum of patients who could benefit. Because the screen was run across molecularly profiled lines, the data can also be used to build biomarker hypotheses. Fibronectin (FN1) expression, for example, negatively correlates with sensitivity to FAK, SRC and MEK inhibitors across the panel, a relationship consistent enough to be worth testing prospectively across a larger cohort.
From screening to translation
Neil and colleagues have made the full dataset available, including raw image analysis outputs, plate maps, dose-response data and validated hit lists with target annotation. For Neil, this study is just the starting point:
“We are planning to test our hits across a wider panel of GBM stem cells, in combination with each other and with standard-of-care therapy such as radiotherapy and temozolomide. It is our view that drug combinations targeting GBM stem cells will move the needle in terms of more effective and durable responses across a wider population of GBM patients.”
More broadly, the study reflects a shift in how drug discovery is approached in glioblastoma. Rather than searching for activity in a single model and hoping it generalises, this work treats heterogeneity as a starting point, using it to identify mechanisms of action that are effective across diverse cellular states. In a disease defined by variability, that change in approach may prove as important as any individual target or compound.
