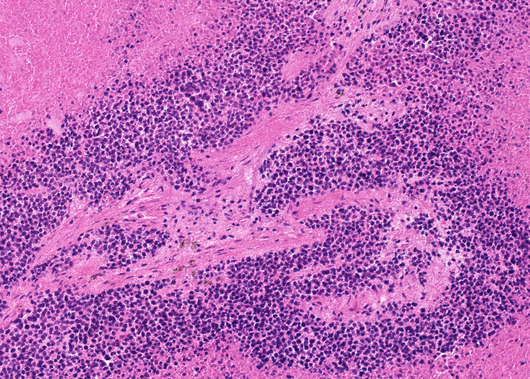
HCI-028 breast cancer PDX
HCI-028 PDX: One of many Patient Derived Xenografts providing breast cancer models including endocrine-resistant estrogen receptor-positive (ER+).
Contributors
| Inventor | Institute |
|---|---|
| Alana L Welm, Yi-Chun Lin, Yoko Sakata DeRose | The University of Utah Research Foundation |
| Cat. #: | 162094 |
|---|---|
| Cancer types: | Breast cancer |
| Cancer Subtype: | Infiltrating Ductal Carcinoma |
| Gender: | Female |
| Biopsy Site: | Pleural Effusion Fluid |
| Patient ethnicity: | Caucasian |
| Treatment History: | Pretreated: Patient had undergone radiation therapy of breast in 2011 and had received systemic treatment of doxorubicin, cyclophosphamide, paclitaxel 2011; tamoxifen 2011; metformin trial 2014-2015; letrazole 2015; zolendronic acid 2015 (1 dose); pertuzumab, trastuzumab, taxotere 2015; everolimus and exemestane2015; capecitabine, lapatinib 2015; docetaxel 2016; pertuzumab, trastuzumab 2016; ado-trastuzumab emtansine 2016; methotrexate 2016; topotecan 2016 prior to sample collection |
| Primary citation: | Guillen, et al. 2022. Nature Cancer. Feb; 3(2):232-250. PMID: 35221336 |
| Product description: | Human breast cancer patient-derived xenograft (PDX) model that retains high fidelity to original tumour, including spatial structure, intratumour heterogeneity, genomic features, tumour growth rate, metastatic patterns, and drug responses. These highly translatable PDX models can be used to more accurately assess therapeutic efficacy and predict patient responses in preclinical drug validation studies than traditional models. This panel of PDX models includes some of the deadliest forms of breast cancer such as drug-resistant, metastatic tumours, and endocrine-resistant estrogen receptor-positive (ER+) and human epidermal growth factor receptor positive (HER2+) tumours. Sample collected in 2016 from pleural effusion of Caucasian female, age 31 at time of collection with a primary diagnosis of IDC; 2010. Patient was a former smoker for 10 years, and had clinical metastasis detected in bone, lung, ovary, liver, and brain. Patient had undergone radiation therapy of breast in 2011 and had received systemic treatment of doxorubicin, cyclophosphamide, paclitaxel 2011; tamoxifen 2011; metformin trial 2014-2015; letrazole 2015; zolendronic acid 2015 (1 dose); pertuzumab, trastuzumab, taxotere 2015; everolimus and exemestane2015; capecitabine, lapatinib 2015;docetaxel 2016; pertuzumab, trastuzumab 2016; ado-trastuzumab emtansine 2016; methotrexate 2016; topotecan 2016 prior to sample collection. Patient and PDX characteristics were as follows – ER status: negative, PR status: negative, HER2 status: negative. PDX information: PAM50 subtype is HER2-enriched and metastasis in lymph node, lung, and liver detected. |
|---|
| Initial handling information: | Implant into the cleared inguinal mammary fat pad of female Immune-compromised mice NSG and NRG. Both NSG and NRG (fresh) time to growth: 5 months to 2 cm |
|---|---|
| Additional notes: | Additional Information on PDX establishment: https://www.nature.com/articles/s43018-022-00337-6/figures/9 |
| Mice Passaged: | Yes |
|---|---|
| Engraftment Site: | Cleared mammary fat pad |
| Host Strain: | Immunocompromised mice NOD scid gamma (NSG) Jackson Laboratory 5557; NOD/scid, Jackson Laboratory 1303 or NOD rag gamma (NRG), Jackson Laboratory 7799 |
| Histology: | PAM50 subtype Her2 enriched |
| Production details: | Fresh or thawed human breast tumour fragments were implanted into the cleared inguinal mammary fat pad of female Immune-compromised mice. For bone metastasis samples, bone fragments were coimplanted. For liquid specimens, pleural effusion, or ascites fluid, 1-2 milion cells were injected into cleared mammary fat pads in Matrigel. For ER+ tumours, mice were dosed with E2 beeswax pellets and given supplemental E2 via drinking water. When tumours reached 1-2 cm in diameter, tumours were aseptically collected and reimplanted into new m ice or banked. Estrogen-independent ER+ breast PDX models were generated when ER+ PDX tumours were transplated into overiectomized mice without E2 supplementation. |
| References: |
Tufail, et al. 2024. Journal of Translational Med. Jan 3:22(1):15. PMID: 38172946 Bhattacharya, et al. 2023. Journal of Experimental & Clinical Cancer Research. Dec 16:42(1):343. PMID: 38102637 Prekovic, et al. 2023. EMBO Molecular Medicine. Dec 7:15(12):e17737. PMID: 37902007 Daneshdoust, et al. 2023. Cells. Sep 30:12(19):2338. PMID: 37830602 Wang, et al. 2023. Cell Bioscience. Dec 1:13(1):224. PMID: 38041134 Guillen, et al. 2022. Nature Cancer. Feb 3(2):232-250. PMID: 35221336 |
|---|
Related Tools for PDX models
| Cat. # | Tool Name | |||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 151146 | Anti-p53 [Pab 240] |
Key Info
Anti-p53 [Pab 240]
|
View Tool | |||||||||||||||||||
| 153247 | fR5 Cell Line |
Key Info
fR5 Cell Line
|
View Tool | |||||||||||||||||||
| 160878 | p27 kip1 [SX53G8.5] |
Key Info
p27 kip1 [SX53G8.5]
|
View Tool | |||||||||||||||||||
| 162073 | HCI-005 breast cancer PDX | View Tool | ||||||||||||||||||||
| 162079 | HCI-011 breast cancer PDX |
Key Info
HCI-011 breast cancer PDX
|
View Tool | |||||||||||||||||||